Request Demo
Last update 08 May 2025

Sindh Institute of Urology & Transplantation
Last update 08 May 2025
Overview
Related
NCT05617378
Exploring the Risk Factors for Colorectal Cancer in Our General Population Using Asian Pacific Screening Score: a Survey From Pakistan
NCT05463276
The Characteristics and Risk Factors of Breast Cancer Patients Trend Distinctive Regional Differences: a Cross-sectional Study
NCT05996588
Comparison Between Inhalational Anesthetic (Sevoflurane) and Intravenous Anesthetic (Propofol Infusion) for Maintenance of Sedation During Endoscopic Retrograde Cholangiopancreatography
100 Clinical Results associated with Sindh Institute of Urology & Transplantation
Login to view more data
Login to view more data
08 Apr 2025Neurology
Comparing Efficacy and Safety of Levetiracetam Versus Phenytoin in Brain Injury: An Umbrella Review (P6-4.004)
Author: Shahab, Azka ; Abbasi, Sassi ; Chaudhary, Esha ; Sohail, Muhammad Ahmad ; Zulfikar, Aimen ; Maryam, Areeba ; Qadri, Syeda Nimra ; Aimen, Sania ; Saeed, Zunaira ; Abideen, Zain ; Waseem, Hassan ; Deepak, FNU ; Lucke-Wold, Brandon
01 Apr 2025Clinical Microbiology and Infection
Incorporating ethics into infectious disease clinical practice guidelines
Review
Author: Zanchi, Chiara ; Righi, Elda ; Jamrozik, Euzebiusz ; Akova, Murat ; Shirin, Neta ; Rodríguez-Baño, Jesús ; Nagavci, Blin ; Armellini, Maddalena ; Nasim, Asma ; Barac, Aleksandra ; Yahav, Dafna ; Tunali, Varol ; Paño-Pardo, José Ramón ; Scudeller, Luigia
01 Apr 2025JACC: Advances
Comparative Congenital Cardiac Catheterization Registry Analysis From the United States and Low- and Middle-Income Countries
Article
Author: Boe, Brian A ; Hasan, Babar ; Ali, Fatima ; Yeh, Mary J ; De Decker, Rik ; Polivenok, Igor ; Bergersen, Lisa ; Lozier, John ; O'Byrne, Michael L ; Kumar, Raman Krishna ; Kreutzer, Jacqueline ; Jenkins, Kathy ; Walshe, Fiona E ; Quinn, Brian P ; Barry, Oliver M ; Ronderos, Miguel ; Holzer, Ralf J ; Gauvreau, Kimberlee
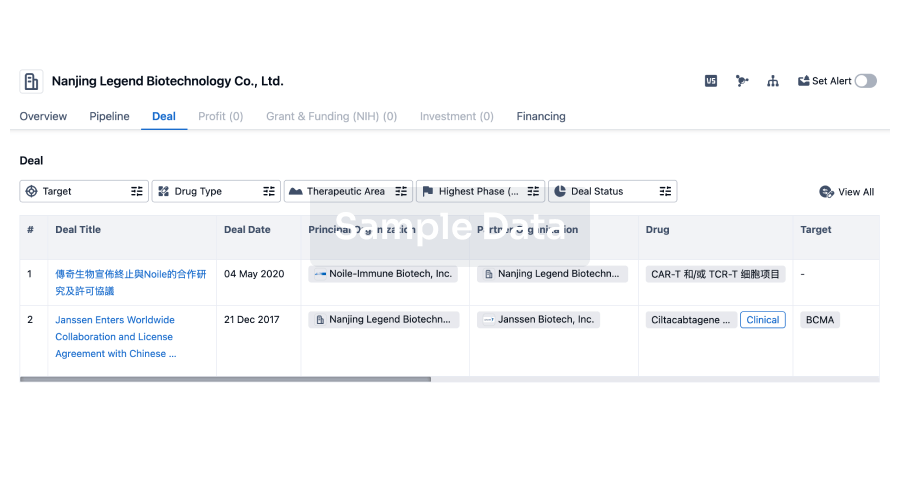
100 Deals associated with Sindh Institute of Urology & Transplantation
Login to view more data
100 Translational Medicine associated with Sindh Institute of Urology & Transplantation
Login to view more data
Corporation Tree
Boost your research with our corporation tree data.
login
or

Pipeline
Pipeline Snapshot as of 19 Dec 2025
No data posted
Login to keep update
Deal
Boost your decision using our deal data.
login
or
Translational Medicine
Boost your research with our translational medicine data.
login
or

Profit
Explore the financial positions of over 360K organizations with Synapse.
login
or

Grant & Funding(NIH)
Access more than 2 million grant and funding information to elevate your research journey.
login
or

Investment
Gain insights on the latest company investments from start-ups to established corporations.
login
or

Financing
Unearth financing trends to validate and advance investment opportunities.
login
or
AI Agents Built for Biopharma Breakthroughs
Accelerate discovery. Empower decisions. Transform outcomes.
Get started for free today!
Accelerate Strategic R&D decision making with Synapse, PatSnap’s AI-powered Connected Innovation Intelligence Platform Built for Life Sciences Professionals.
Start your data trial now!
Synapse data is also accessible to external entities via APIs or data packages. Empower better decisions with the latest in pharmaceutical intelligence.
Bio
Bio Sequences Search & Analysis
Sign up for free
Chemical
Chemical Structures Search & Analysis
Sign up for free